Les défis de l'intégration des technologies d'assistance dans les services de soins aux personnes âgées Une étude comparative du Japon et de la Finlande
- Type de publication : Article de revue
- Revue : European Review of Service Economics and Management Revue européenne d’économie et management des services
2018 – 2, n° 6. varia - Auteurs : Watanabe (Kentaro), Hyytinen (Kirsi), Tuovila (Hannamaija)
- Résumé : Le vieillissement constitue un défi mondial. Alors que les TIC et la robotique sont envisagés comme des solutions pour des soins durables, leur intégration dans les systèmes de services de soins aux personnes âgées est difficile. Cette étude porte sur les services de soins en établissement au Japon et en Finlande. En s’appuyant sur des entretiens auprès de gestionnaires de ces services, l’étude a clarifié leurs attentes à l'égard des technologies et les obstacles à l'intégration de celles-ci.
- Pages : 97 à 122
- Revue : Revue Européenne d’Économie et Management des Services
- Thème CLIL : 3306 -- SCIENCES ÉCONOMIQUES -- Économie de la mondialisation et du développement
- EAN : 9782406086338
- ISBN : 978-2-406-08633-8
- ISSN : 2555-0284
- DOI : 10.15122/isbn.978-2-406-08633-8.p.0097
- Éditeur : Classiques Garnier
- Mise en ligne : 15/10/2018
- Périodicité : Semestrielle
- Langue : Anglais
- Mots-clés : Vieillissement, soins aux personnes âgées, système de service, technologie d'assistance, comparaison
Challenges in Integrating
Assistive Technologies
into Elderly Care Services
Comparative Study
between Japan and Finland1
Kentaro Watanabe
National Institute of Advanced Industrial Science and Technology
Kirsi Hyytinen,
Hannamaija Tuovila
VTT Technical Research
Centre of Finland Ltd
Introduction
The aging of population has caused serious, global challenges towards elderly care service systems. One of the challenges is an increasing public expenditure. There is limited working population to pay rising public expenditures caused by increasing demands for health and social welfare services. Every OECD country will face substantial increase of public expenditure for elderly care, especially long-term care, corresponding to the increase of older people. (de la Maisonneuve and Martins, 2013). 98Not only financial sources, but also various kinds of resources for care, such as professional caregivers and family caregiving will be required more, which has raised a question about the sustainability and quality of care services.
Recently, ICT and robotic technologies have been actively developed and introduced to support care services and the life of the elderly (Sun et al., 2009; Obi et al., 2013; Sugihara et al., 2015). These technologies are expected to be a potential solution to the challenges caused by aging. As a research field focusing on technology development for the challenges of aging, gerontechnology aims at finding technological solutions which improve the daily functioning and the quality of life of the elderly (Pieper, 2002; Bouma and Graafmans, 2008). It is becoming increasingly important to develop solutions, which facilitate social support for the elderly, improve workforce availability and make the elderly care services more cost effective for healthcare systems (Siegel et al., 2014). One of the main challenges in gerontechnology is to support the independent living of elderly people while reducing the burden for themselves, national health systems, insurance companies, relatives and care personnel (Sale, 2018). The support of the independent living of the elderly is highlighted also in the research on Ambient Assisted Living or Active and Assisted Living (AAL). AAL research aims at developing new concepts, products and services to support the daily living at home, by combining ICTs and social environments (Siegel et al., 2014). More recently, care robotics are gaining attention as new potential solutions for challenges in elderly care. For example, therapeutic effects of social robots such as Paro have been investigated and applied to actual care environments (Shibata and Wada, 2011). An exoskeleton device for physical support is also a typical technology application to recover the physical ability of a care recipient and to reduce the burden of a caregiver (Kawamoto and Sankai, 2005).
While a variety of technologies have been developed, introduction and integration of them into elderly care service processes are still cumbersome. A technological solution tends to be inadaptable to different situations of the elderly and the people working with them (Leikas, 2014). Not only technology development, but also service innovation are necessary to address the societal challenge of aging (Gallouj et al., 2015). Technology is a part of resources required for service systems (Edvardsson and Olsson, 1996). For service innovation utilizing novel 99technologies, the overall arrangement of service systems including different types of actors needs to be considered (Edvardsson and Olsson, 1996; Sundbo, 1997; Gallouj and Weinstein, 1997).
This study specifically focuses on international contexts of technology use for elderly care. Each country has its own care policy, management and culture for elderly care (OECD, 2005, 2013), which affects requirements for technologies and their integration process. The international comparison of care policies and practices have been conducted in many studies (OECD, 2005; Campbell et al., 2010; Rhee et al., 2015). However, few studies focus on the impact of the differences among countries, concerning technology integration and diffusion in elderly care service systems. Expected roles of technologies in elderly care service systems would be different in each country. By understanding these differences, the integration and diffusion process of technologies will be more sophisticated, and then the technologies will be more integrated in service practices and the life of the elderly in a way to increase the quality of life (QoL) of the elderly and their families, and the quality of work (QoW) of care personnel.
In this study, we aim at clarifying how the expectations towards new technologies and their integration differ between Finnish and Japanese elderly care service systems. Both countries have high ratios of aged population and have already confronted challenges caused by aging (OECD, 2013). Our specific focus is on facility care services. Although home care tends to be highlighted based on the concept of “aging in place” (OECD, 2005), facility care also requires innovations through integration of new technologies to support the life of the elderly, especially with memory illnesses and heavy disabilities. Through the analysis, the requirements and challenges of technology integration to different elderly care service systems will be obtained.
The contents of this paper are as follows. In section 2, we explain the service system perspective as an analytical framework for the comparative study of elderly care services. In addition, we introduce the overview of elderly care policy and services in Japan and Finland. In section 3, we explain the research methodology and cases of this study. We present the findings from the interview study in section 4 and provide some implications and limitations in section 5. Finally, we provide concluding remarks in section 6.
1001. Background
The service system perspective is a natural way to approach solutions and innovations in elderly care services, which are organized among different types of actors. In the recent literatures, framing and conceptualizing innovation in the health and social welfare service sector have been one of the focus areas (e.g., identification of new service concepts, new customer interaction, new value system/business partners, new revenue models, new organizational or technological service delivery systems) (den Hertog, 2010). Also, co-creation of services with customers has been topical in recent years (Elg et al. 2012; Witell et al. 2011). In addition, some of the scientific advances on the service innovation theories (Gallouj, 2002; Windrum and García-Goñi, 2008) have been developed based on examples from the health and social welfare sector.
In this paper, we adopted several perspectives which are relevant to characterising the elderly care service system. These are multi-actor interactions, socio-technical nature and institutions (Watanabe et al., 2016).
1.1. Service system and multi-actor
approach in elderly care
According to Edvardsson and Olsson (1996), a service system consists of different types of resources that are available for realizing a service. There are four types of resources; the service organization’s staff, the customers, the physical/technical environment, and organization and control. Määttä et al. (2016) applied this framework to analyze the impact of technologies towards the elderly care service system as shown in Figure 1. The first resource, the service organization’s staff is seen as a key resource. A service is realized in the interaction between the customer and the staff. In the elderly care context, the service organization’s staff is care personnel providing care for the elderly. The second resource, the customers, are the elderly themselves and their family members. Edvardsson and Olsson (1996) highlighted that the customers in the service system are contributors in the service process, 101not just participants. This idea is also in the core concept of value co-creation in Service Dominant Logic (SDL) (Vargo and Lusch, 2004, 2011). This should be taken into account when developing solutions to the service system. The third resource, the physical/technical environment, includes any kinds of facilities and technical systems, such as computers at service premises. In the elderly care context, these are, for example care facilities and their technological equipment. According to Edvardsson and Olsson (1996), the physical/technical environment should not be a goal for development but should be a means for providing better services. The fourth resource, organization and control is, in the elderly care context, the care organization which includes its organizational structure with activities and responsibilities, internal processes and organizational support systems. All these resources must function together to realise the service concept, i.e. the value for customers. This means that introducing new technologies such as ICT and robotics affects the whole service system.
The active role of actors, especially customers is strongly emphasized when the necessity of resource integration is brought to the fore. SDL theorized by Vargo and Lusch (2004, 2011) defines ‘service’ as a process of using one’s competences (knowledge and skills) for the benefit of another party. SDL includes several implications for the development of elderly care service systems. The reciprocal nature of the interaction among actors implies that the elderly are not just the recipients of services, but they function as active agents and a resource in service provision. SDL takes service as a ubiquitous, collaborative process in a system of variety of actors. In service innovation, it highlights the role of institutions which are discussed later, and social structures that guide the action and interaction between multiple actors (Vargo et al., 2015; Wieland et al., 2012). Technology becomes meaningful only when it is linked to other resources and its value is always defined by its user.
102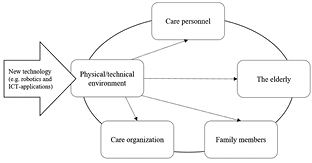
Fig. 1 – Resources in the elderly care service system
(Määttä et al., 2016; adapted from Edvardsson and Olsson, 1996).
Elderly care is coordinated and sustained by multiple actors (Djellal and Gallouj 2006). The studies on service systems highlight the importance of multi-actor interactions in value creation processes. Actors inside a health organization play an important role in innovation generation and dissemination. Frontline workers and their managers should be motivated and skilled enough to ensure a successful implementation of innovation (Windrum, 2013). Integration of customers and external networks has been emphasized in realizing service innovations (Edvardsson and Olsson, 1996; Sundbo, 1997; Sundbo and Gallouj, 2000). Gallouj and Weinstein (1997) theorized multiple actors’ relationship in service systems and an assessment method from their perspectives, as multi-actor framework. This framework has been adopted especially to public services and Public-Private Partnership. For example, Windrum extended this framework to social innovation processes (Windrum, 2013; Windrum et al., 2016). In the elderly care service system, the key actors are the elderly, their family members, care personnel and managers of care organizations. But also, external stakeholders should be taken into account, such as municipalities, third sector organisations and technology developers and integrators (Watanabe et al. 2017).
1031.2. Socio-technical nature
and institutions in elderly care
In this study, technologies are applied to service systems, which create value through interactions among actors. Development of technologies provides new opportunities, not only for the solution of elderly care issues, but also for the introduction of new collaboration practices that increase the efficiency and effectiveness of elderly care, i.e. reduction of the costs and improvement of service quality. These practices include both the interaction between care personnel and the elderly, and the inter-organizational and cross-functional interaction among service providers. Figure 1 intends to represent physical/technical environment as the major resource in the elderly care service system. In this sense, the socio-technical perspective is essential in this study to specify the role of technology in elderly care service systems. Technology developers or integrators are required to understand the service system to apply a new technology to the system, which is depicted as an arrow in Figure 1.
In addition, a large-scale change through technology integration in a service system is also not straightforward. The simultaneous development of organisations, technologies, services and multiple network relationships are required for such a large-scale change (Gallouj, 1994, 2002; Windrum and García Goñi, 2008; Harrison et al., 2010). Furthermore, it is essential to understand the whole socio-technical system, including the dynamic interplay between parts of the system as well as the social support and social engagement, for realizing the system level solutions (Geels, 2002, 2004).
This study investigates elderly care service systems in two different countries. For the analysis from the international viewpoint, this study focuses on institutions in service systems. Scott (2001) illustrates institutions which “comprise regulative, normative, and cultural-cognitive elements that, together with associated activities and resources, provide stability and meaning to social life.” Institution includes explicit and implicit rules, norms, regulations, customs and common behaviours. They affect not only organizational behaviours, but also value creation processes in service systems (Vargo et al., 2015). Akaka et al. (2013) specifically emphasize the importance of institutions in service ecosystems in the international settings. Since technology is a part of service systems, institutions could also affect the role of technologies in elderly care services. We adopted institutions as a part of the analytical framework in this study.
1041.3. Overview of elderly care
in Japan and Finland
The Japanese population is 127.0 million and is approximately 23 times more than Finland’s population of 5.5 million (World Bank, 2018). Concerning the aging situation, Japan has the highest ratio of the over 65-years-old population, which was 26.6 % in 2016 (World Bank, 2018). Although Finland has smaller ratio than this, it has already been 20.8 %, which is higher than the average of OECD member countries, which in 2016 was 16.5 % (World Bank, 2018). Finland and Japan are both highly aged countries and share the same challenges of aging population.
In Table 1, we summarize the current characteristics of elderly care in Japan and Finland. Regarding the elderly care policies, the two countries differ quite a lot. Japan has adopted a Long-Term Care (LTC) insurance system, which was activated in 2000. In this system, it is mandatory for citizens over 40-years-old to pay a premium, and citizens over 65-years-old can be beneficiaries in principle to receive elderly care services (Hayashi, 2014). Recipients of elderly care services have to pay 10-20 per cent of the care expenses by themselves, according to their income. The total amount of the insurance payment is determined based on the assessment held by municipalities. The LTC expenditure (health and social components) by government and compulsory insurance schemes per GDP in 2014 was 2.0 % (OECD, 2017). The aging of baby-boomers will cause rapid increase of public expenditure, which could reach to 19.8 trillion yen in 2025 (Fujishiro, 2015). Therefore, the reform of the care system has been continuously conducted to hold down the increase (Shimizutani, 2013; Hayashi, 2014). In Finland, the elderly care system is characterized by the Nordic Welfare Model, in which universal services are provided by strong public sectors based on tax funding (Teperi et al., 2009). Elderly care service is provided according to the assessment conducted by a municipality. The main financial resources are subsidies from the government and taxation by local municipalities. Except the basic services, municipalities are also allowed to charge users directly. The LTC expenditure (health and social components) by government and compulsory insurance schemes per GDP in 2015 was 2.2 % (OECD, 1052017). The estimated future financial status is not at the satisfactory level. Therefore, for these several years, the renewal of the social welfare and health care system has been discussed to innovate the existing municipality-based service structure for ensuring equal and adequate services for citizens (THL, 2018).
In Japan, facility care services (except residential services with home care and group homes for dementia) can only be provided by organizations authorized by prefectural governments. They are private, non-profit organizations (Hayashi, 2014). The elderly and their family can choose any service in principle, although the elderly need a sufficient care need level for 24-hour care, which is determined by the municipal assessment. While a municipality in Japan acts mainly as an insurer (Hayashi, 2014), municipalities in Finland take more responsibility in providing services. Recently, small and financially weak municipalities in Finland have encountered difficulties in organizing and providing the services, which is why it is discussed in the reform that the responsibility for providing social welfare and health care services will be transferred to larger administrative entities by the year 2020 (THL, 2018). There are both public and private services in Finnish facility care for the elderly. The role of the private social and healthcare sector is growing. They offer hospital services, senior home accommodation and home care services for the elderly, such as call-centre services, meal services, cleaning and security services. However, even when private services are used, the municipalities generally procure their services and provide them to the users (OECD, 2013). The Finnish municipalities decide necessary care services for each elderly person according to an assessment. Recently, a service voucher system has been adopted in large municipalities, which allows the elderly to choose services they need (Anttonen and Karsio, 2016). Although the freedom of choice in Finland is currently smaller than in Japan, one of the main goals of the ongoing social welfare reformation is to increase the freedom to choose among different public and private service providers, also in the case of elderly care services (Alueuudistus, 2017).
106|
Japan |
Finland |
|
|
Population (Year 2016) |
127.0 million |
5.5 million |
|
Ratio of 65Y over |
26.6 % |
20.8 % |
|
Elderly care system |
Long-term care insurance |
Nordic welfare model |
|
Service charge |
10 % (20 % if the income level is high) |
Varies according to a municipality, service form and service provider |
|
Public expenditure for LTC per GDP |
2.0 % (Year 2014) |
2.2 % (Year 2015) |
|
Service providers |
Mainly private |
Mainly public |
|
Freedom of choice |
Large |
Small, but increasing |
|
Role of the municipality |
Insurer |
Responsible in organizing services (will be transferred to counties) |
Tab. 1 – Current characteristics of elderly care in Japan and Finland
(World Bank, 2018; OECD, 2017; Niemelä et al., 2017).
While Japan and Finland are the ones of the most aged countries, there are a variety of differences in their demographics, policies and institutions. The comparison between these two countries does not aim at bringing focused implications, but rather exploring multi-faceted aspects affecting technology integration in the elderly care service systems. The results will be beneficial not only for Japan and Finland, but also for other countries which share parts of characteristics in them and their elderly care service systems.
1072. Methodology
To get an overview on the expectation and role of technologies at elderly care facilities, we conducted an interview study to top-level or middle-level managers. For the purpose of our study, we especially focused on two points: (1) what kind of technology is being used or expected, (2) what kinds of challenges exist in integrating technologies into service systems for different types of actors. We conducted seven semi-structured interviews with managers in facility care service providers both in Japan and Finland. Altogether, we conducted 14 interviews. Table 2 summarizes the interviewee profiles.
Interviews in Japan were held between March and April in 2016. Interviews in Finland were held during November 2016 and May 2017. The interviewees were selected by the opportunistic sampling but this study covered a variety of facility sizes and forms of facility care (general care, care for memory illness). Japanese interviewees were only from private organizations (including both for-profit and non-profit organizations), due to the fact that Japanese facility care services are mostly provided by the private sector. In Finland, the interviewees consist of both public and private organizations.
|
No. |
Interviewee in Japan |
No. |
Interviewee in Finland |
|
J1 |
Facility manager of a facility in a large healthcare and elderly care corporation (no voice recording) |
F1 |
Executive director of a small non-profit organization operating a care home |
|
J2 |
CEO of a large healthcare and elderly care corporation |
F2 |
Executive director of a care home, owned by a foundation |
|
J3 |
Managing director, a large healthcare and elderly care corporation |
F3 |
Director of communication, a large international care service company |
| 108
J4 |
CEO of a small group home for dementia |
F4 |
Facility manager of a care home, operated by a large international care service company |
|
J5 |
CEO of a large elderly care corporation |
F5 |
Facility manager of a care facility for memory illnesses, operated by a municipality |
|
J6 |
CEO of a small group home for dementia |
F6 |
Facility manager of a care home for memory illnesses, operated by a company (no voice recording) |
|
J7 |
Executive Head of a large social and welfare corporation |
F7 |
Facility manager of a care home, operated by a municipality |
Tab. 2 – Summary of interviewee profiles.
The interview time differed between 60 to 120 minutes. All of the interviews were recorded and transcribed, except in two interview cases where voice recording was not applicable. Interview notes were also used to supplement the gathered data. The interview language in Japan was mostly Japanese. The interviewer talked through a translator, who was a member of the research project. The interview languages in Finland were both English and Finnish. When the interviewee could communicate in English, we only used English, but when the interviewee was not fluent enough in English, we communicated through a translator. Though we trust that our translators were able to translate the most essential parts of the interviews for the purpose of our study, it should be noted that some parts of the interviews might have been filtered out during the translation process.
1093. Findings
Interview results illustrated both similarities and differences about expectations and challenges toward technology integration, between Japan and Finland. The barriers for technology integration mentioned in the interviews were mostly common in both countries, while some different aspects were observed. Meanwhile, there were substantial differences, especially about expectations toward new technologies.
3.1. Technologies in use
In Japan, some of the interviewed care facilities had implemented different types of care recording systems, which were used especially for requesting insurance payments. The care facility under the healthcare corporation had an access to the electronic health record (EHR) also. Another technology in use was an automatic bathing support system, which supports the care personnel in helping the elderly who have difficulties in moving, to take a bath safely. The cultural aspect of the technology should be highlighted here. Taking a bath is very important in the Japanese culture. Most of Japanese people take a bath every day. With this kind of support system, it becomes possible to provide a bathing experience also for the elderly with disability which does not allow them to take a bath. The bathing culture of Japan is comparable to the Finnish sauna culture. Sauna is a part of the Finnish identity, a place for peace and quiet, and something people grow up with. This is why there is a sauna in almost every interviewee’s facility in Finland, although it does not necessarily require specific technological devices to help the elderly get in.
In Finland, most of the interviewees reported that they used ICT for care personnel to record results of care services and to communicate among care personnel. Several interviewees answered that they used the common ICT tool to assess long-term physical and psychological change of their clients. Public facilities had an access to the EHR of the municipality which they belong to, but private facilities did not necessarily have an access to the municipality’s system. Private facilities use the municipal EHR indirectly through the visiting medical doctors, and the facilities use 110their own messaging or care recording systems. A lifting device to transfer a resident from a bed to a (wheel) chair or vice versa, is another common technology used in the interviewees’ facilities. One interviewee reported that they used a work scheduling software in the facility, with which a care professional can negotiate the change of their work shift with another.
3.2. Expectation towards new technologies
In the interviews in Japan, reducing the burdens of care personnel was strongly emphasized. Technologies which can support care personnel, such as wearable robotic lifting devices were mentioned as expected technologies, while the existing lifting devices were not highly evaluated. One interviewee said “In Japan, most facilities don’t use lifts. …Using lift could be better but, maybe it’s not kind to elderly people. That’s what many of my co-workers say.” Meanwhile, one interviewee also said that the current robotic lifting device looked ‘gigantic’ and required improvement. As another supportive technology, monitoring and alert systems which can detect residents’ movement at night and outgoing residents were taken up. In addition, one interviewee mentioned a mobile information sharing system for care personnel for daily reporting and knowledge sharing. Some interviewees show their expectation toward care robots, which can communicate with the elderly, for example; “The residents get older and have more difficulty in doing something, so a lot of care is needed. … More communication is required for the elderly people, but it’s something difficult. In that case, the communication robots will do the effect.”
In Finland, systems to increase safety of residents such as a bed monitoring system were most commonly mentioned as an expected technology. This is the common technology expected in both countries. Such a monitoring technology can improve the safety of the elderly and also reduce the cost to check the situation of the elderly, especially in the night shift. In addition, the interviewees in Finland generally preferred back-office technologies such as a logistics system inside a facility and an automatic work scheduling system.
Several interviewees in Finland considered care robots which directly contact with the elderly as negative. Some interviewees had already tested care robots in their facilities. One interviewee mentioned her experience as “There’s also a mental thing in Finland. I would think that there would be a lot of discussion about the ethics. … The robot is taking care of our elderly. 111In Finland, that’s a bad sentence.” Meanwhile, one Finnish interviewee was very positive in care robot which directly contacts with the elderly.
3.3. Barriers to integrate technologies
in care services
The interviewees mentioned potential and actual barriers to integrate technologies in care services as follows. Table 3 summarizes these barriers and the actors related to them for each country.
Change in work
Some of the interviewees in both countries felt it a challenge to change the mind-set of care personnel to use technologies at work. Integration of technologies in work causes the change of workstyles, which made care personnel reluctant to accept technologies, one interviewee in Japan stated. The reluctance to change the workstyle was mentioned in relation with the older age of care personnel in both countries, such as “Currently the average age of the employees is over 40. So, there are many 50s, 60s, and even 70s. For them it’s rather difficult to adapt to such kind of new technologies, and they are reluctant to change their working styles.” One interviewee in Japan mentioned another potential challenge which came from the lower educational background of care personnel. Meanwhile, one interviewee in Finland suggested that the intergenerational interactions had helped to introduce technologies at work. In her facility, the younger personnel taught how to use new technologies to the older, and the older personnel taught the experience in care to the younger, which made a good cycle in the workplace. Some interviewees in Finland mentioned that the manager’s positive attitude toward technologies would affect care personnel’s willingness to technology use.
Immature technology
Immature technologies and their interfaces also affected the acceptability of technologies for care personnel, which was mentioned in both countries. In Japan, several interviewees mentioned that the time to 112use technologies was a challenge to overcome, especially about the use of the lift. There was another comment from one interviewee that the current robotic wearable lifting device was not also considered suitable to the care setting, as was written above.
“Care-by-hand” culture
Another challenge is a “care-by-hand” culture. One interviewee in Japan mentioned that the mindset that care should be done by hand made care personnel reluctant to use technologies, like “We, people who worked for this area, tried to become more like a family, or very warm-handed. … We have the cultural belief or, we tend to think that, doing everything manually or doing by the hand is very nice for elderly people.” The same kinds of arguments were stated in Finland also, but rather it was mentioned as the management policy from the aspect of humanity. In their view, human relationship should be highly respected concerning care.
Public image toward robotics
One interviewee in Finland mentioned the public image toward technologies, specifically care robots, based on his experience. The interviewee depicted the image toward robotics in care as “One trouble with robotization and with usage of technology, because it’s not depicted as warm. It’s not human. It’s like that. It’s cold. It’s violent. It’s, in a marketing way, bad.” This type of notion from the public viewpoint was not heard in the interview in Japan.
Privacy
Although monitoring and alert systems for the safety of residents were expected in both countries, it was not necessarily preferred to use videos for monitoring. Some interviewees in Finland were negative about video monitoring, from the aspect of privacy. One interviewee in Japan also said, “There is some kind of prevention of falling down. There 113are some systems that take the videos. … I’m against such kind of technologies, like to watch somebody or such kind of things. … I don’t want to change the policy to keep the human to human relationship in a way.”
Cost of technologies
From the managerial perspective, the cost for new technologies is a big barrier to implement them in both countries. Especially for the interviewees in smaller facilities, it is difficult to compensate the cost of technologies.
Limited impact in management
One interviewee in Finland stated the investment toward technologies did not help management, because the number of care personnel required for services is fixed by law. This situation was the same in Japan. Meanwhile, one interviewee in Japan mentioned that increasing the work safety of care personnel with technologies would be beneficial from the managerial perspective.
|
Challenges |
Main actors |
Japan / Finland |
|
Change in work |
Care personnel |
Both |
|
Immature technology |
Care personnel, |
Both |
|
“Care-by-hand” culture |
Care organization, |
Both, with different views between Japan and Finland |
|
Public image toward robotics |
The elderly, family |
Finland |
|
Privacy |
The elderly, family |
Both |
|
Cost of technologies |
Care organization |
Both |
|
Limited impact to management |
Care organization |
Both, but with a positive view in Japan |
Tab. 3 – Barriers to integrate technologies in care facilities.
1144. Discussion
The findings from the interviews highlighted the importance of multi-faceted understanding of elderly care service systems for integrating technologies into them. Especially requirements and expectation toward technologies were affected by the characteristics of the service systems including institutions. We also specified common challenges for assistive technologies and approaches to integrate technologies to facility care services. We further discuss these issues from the aforementioned three theoretical perspectives.
4.1. Requirements and challenges
from multi-actor perspective
Regarding the technologies in use and the expected technologies, we were able to specify some similarities and differences between both countries. Concerning ICTs to record and share care information, municipalities in Finland are responsible in providing services, so they can lead technology integration toward multiple facilities in their region. Meanwhile, there were some differences in technology use between private and public service providers. In Japan, facilities owned by private organizations need to take care of their own services, which might cause slower diffusion of standardized systems. For such service systems with different care management concepts, different strategies are needed to integrate and diffuse technologies. For example, Ministry of Economy, Trade and Industry (METI) and Ministry of Health, Labour and Welfare (MHLW) in Japan have been subsidizing commercialization and installation of care support devices (Neumann, 2016). Meanwhile, the change by the ongoing social welfare reform in Finland would affect the technology integration pathway. The role of municipality, and upcoming county requires further investigation.
Monitoring and alert systems for residents were mentioned as an expected technology in both countries. This implies that the safety of the elderly is a common issue for the managers in both countries. In addition, reducing the workload to watch over the elderly, especially in 115the night time is also important for both. These are the basic requirements for facility care in both countries, though the acceptability of monitoring methods such as video monitoring can be different in each country or facility according to the management policy.
The interviewees in both countries shared many challenges about integrating technologies. This implies that an effective integration approach in Japan could work at a facility in Finland and vice versa. Meanwhile, for example, different types of “care-by-hand” culture in Japan and Finland would require individual communication and implementation approaches adjusted to managers, care personnel and also the elderly and their families. The precise understanding on the actors’ thoughts is important to configure such an integration process.
4.2. Socio-technical challenge
and institutions affecting
technology integration
The challenge for care personnel to change their work process when integrating technologies shows a typical socio-technical issue in elderly care service systems. The existing studies suggested that participation of stakeholders in both changing their processes and integrating technologies be a successful approach (Greenbaum and Kyng, 1991; Wallin et al., 2015; Watanabe and Mochimaru, 2015). The active role of technology users was emphasized in this study, also. This interview result suggested that the intergenerational support could be also a potential approach for smooth integration of technologies. This type of learning process is meaningful for overall workplaces and requires further investigation through the workplace study.
Institutions are also important for socio-technical change in elderly care service systems, especially when it comes to dynamic, large-scale change. This study revealed several institutional aspects concerning technology integration in the elderly care service systems. First, a culture in the ordinary life of the elderly affects required technologies in each country. As shown in the Japanese case, bathing support technologies are common in care facilities in Japan due to the Japanese bathing culture. Although bathing in a bathtub requires intense support with a heavy-loaded task for care personnel and also contains high risk in safety, it is unavoidable for Japanese care facilities to provide bathing 116services, because it is an important part of people’s life. This type of cultural requirement should be taken into account when exporting technologies to another country.
The culture in care work, specifically the “care-by-hand” culture is another interesting issue in this study. In general, this study showed that the “care-by-hand” culture affected the attitude toward technologies negatively. Meanwhile, the attitudes to each technology are slightly different in each country. In the interview results of Japan, communication between the elderly and robots are expected, while introducing lifting devices is currently challenging. Meanwhile, not only the management policy but also the public reputation could affect the acceptance to care robots negatively in Finland, although lifting devices have been more accepted. These results imply a complex relationship between technological features and each actor’s attitude to them. The findings on the aforementioned cultural aspects in elderly care service systems again emphasized the importance of integrative understanding of each actor’s perspective, as was discussed above.
Laws and regulations also affect the integration of technologies. The regulation on the personnel quota for care could affect the motivation to implement technologies especially for private companies, because there is an expectation that investment toward technologies could contribute to their businesses. One interesting point is that Japanese interviewees have not mentioned this point directly, but rather stressed the benefit for work safety of care personnel. One potential reason of this is that the scarcity of care personnel is serious in Japan (MHLW, 2015) and the improvement of work conditions is considered as an important management issue. Actually, the recent government-funded R&D for elderly care focuses on reducing the burden of care personnel in care facilities (AMED, 2016). This difference implies mixed factors including demographic difference, labour market, work environment and regulations, which could affect the direction of technology development policy.
4.3. Limitation
One of the important limitations of this study is that the interviewees were only managers in facility care services. To supplement other actors’ viewpoints, we have conducted other workplace studies and interview studies, and are preparing further analysis. The number of interviewees 117is also limited to clarify the managers’ general attitudes toward more specific topics, such as the attitude toward care robotics. Meanwhile, this study investigated a variety of aspects which could affect the acceptability and expectations toward technologies. As another limitation, there could be potential biases which come from the opportunistic sampling. In addition, further analysis is needed to evaluate the impact or each barrier collected through interviews when configuring an integration process of certain technologies.
As an international study concerning aging and technologies, we investigated only two countries. To obtain more focused implications based on the results of this study, it will be meaningful to investigate countries with similar service systems, such as Germany with the long-term care insurance policy, and other East Asian countries (China, Taiwan, South Korea, etc.) which are less aged and with the similar cultural background to Japan. For comparing with Finland, other Scandinavian countries will be good candidates. The comparison with US which has significantly different social welfare model both from Japan and Finland could also bring meaningful insights. The insights obtained from these studies would be beneficial for better fit of assistive technologies in each country. This contributes to the wellbeing of the elderly in the global level and also leads to the success of international businesses of technology developers and integrators.
Conclusion
The focus of this study was on expectations and challenges about assistive technologies and technology integration approaches for Japanese and Finnish elderly care service systems. For the comparative analysis, we adopted the service system perspective, which was characterized with multi-actor interactions, socio-technical nature and institutions. Based on this perspective, we conducted the interview study to facility care managers in Japan and Finland.
The results of the interview study showed several common expectations and challenges. Especially, the barriers to integrate technologies in 118care services were widely common between Japan and Finland. It will be meaningful to share experiences to overcome these barriers between the two countries. In addition, the importance of active roles of actors in a service system was also underpinned by the interview result, also.
Concerning the expectation toward technologies, technologies like monitoring and alert systems to tackle the common challenges such as the safety of the elderly, were expected in both countries. Meanwhile, there were also several differences in expectation toward technologies. For example, the physical support for care personnel was more expected in Japan, because the burden of care personnel was considered as a serious challenge in the society. Some of the differences also stemmed from the cultural and regulation factors. The important implication of this study is that the cultural factors affecting technology acceptance should be investigated from each actor’s perspective. For example, the “care-by-hand” culture mentioned in both countries did not necessarily lead to the negative attitude to any kind of technology. The multi-faceted nature of institutions generates complex relationship between technological features and each actor’s attitude to them, and the integration approach should be formulated based on its analysis. The care policy and the role of municipalities in elderly care service systems also affect the pathway to socio-technical change in elderly care. As a practical implication, it is important to clarify these factors and relationship when a technology developer or integrator attempts to apply its technology to different countries. The insights from this study will promote both the success of the assistive technology business and the improvement of elderly care service systems.
The results of this study are limited in the managerial perspective in facility care services. The next step is to integrate and analyse data from the studies on municipalities, care personnel and the elderly to develop the innovation process of elderly care service systems through the integration of technologies. Different types of services such as home care services should be also investigated. In addition, more focused study on the specific technology such as social robots, or countries with similar types of care systems will be interesting research topics in the future. We hope that these studies will contribute to establishing more human-oriented and sustainable elderly care and more independent life of the elderly.
119References
Alueuudistus (2017), “Health, social services and regional government reform website”, available at: http://alueuudistus.fi/en/frontpage (accessed 11 July 2017).
Akaka M. A., Vargo S. L., Lusch R. F. (2013), “The complexity of context: A service ecosystems approach for international marketing”, Journal of Marketing Research, vol. 21, no 4, p. 1-20.
Amed (2016), “Project to Promote the Development and Introduction of Robotic Devices for Nursing Care”, available at: http://robotcare.jp/wp-content/uploads/2016/11/ROBOT-CARE-pamphlet_eng.pdf (accessed on 13.7.2017).
Anttonen A., Karsio O. (2016), “Eldercare Service Redesign in Finland: Deinstitutionalization of Long-Term Care”, Journal of Social Service Research, vol. 42, no 2, p. 151-166.
Bouma H., Graafmans J. (1992), Gerontechnology, Amsterdam, IOS Press.
Campbell J. C., Ikegami N., Gibson M. J. (2010), “Lessons from public long-term care insurance in Germany and Japan”, Health Affairs, vol. 29, no 1, p. 87-95.
de la Maisonneuve C., Martins J. O. (2013), “Public spending on health and long-term care: a new set of projections”, OECD Economic Policy Papers, no 6.
Djellal F., Gallouj F. (2006), “Innovation in care services for the elderly”, The Service Industries Journal, vol. 26, no 03, p. 303-327.
den Hertog P. (2010), Managing service innovation: firm-level dynamic capabilities and policy options, Utrecht, Dialogic Innovatie & Interactie.
Edvardsson B., Olsson J. (1996), “Key concepts for new service development”, The Service Industries Journal, vol. 16, no 2, p. 140-164.
Elg M., Engström J., Witell L., Poksinska B. (2012), “Co-creation and learning in health-care service development”, Journal of Service Management, vol. 23, no 3, p. 328-343.
Fujishiro M. (2015), “Fiscal Consolidation and Debt Management in FY 2015 Draft Budget and Japanese Society in the future”, Japan Securities Summit 2015, London, UK, 11 February.
Gallouj F. (1994), Économie de l‘innovation dans les services, Paris, Éditions L‘Harmattan, Logiques Économiques.
Gallouj F., Weinstein O. (1997), “Innovation in services”, Research policy, vol. 26, no 4-5, p. 537-556.
120Gallouj F. (2002), Innovation in the service economy: The new wealth of nations, Cheltenham and Northampton, Edward Elgar.
Gallouj F., Weber K. M., Stare M., Rubalcaba L. (2015), “The futures of the service economy in Europe: A foresight analysis”, Technological Forecasting & Social Change vol. 94, p. 80-96.
Geels F. W. (2002), “Technological transitions as evolutionary reconfiguration processes: a multi-level perspective and a case-study”, Research Policy, vol. 31, p. 1257-1274.
Geels F. W. (2004), “From sectoral systems of innovation to socio-technical systems: Insights about dynamics and change from sociology and institutional theory”, Research policy, vol. 33, no 6, p. 897-920.
Greenbaum J., Kyng M. (1991), Design At Work: Cooperative Design of Computer Systems, Hillsdale NJ, Erlbaum.
Harrison D., Klein J-L., Browne P.L. (2010), “Social innovation, social enterprise and services”, in Gallouj F., Djellal F. (Eds.), The Handbook of Innovation and Services, Cheltenham and Northampton, Edward Elgar.
Hayashi R. (2014), Social Security in Japan (2014 edition), National Institute of Population and Social Security Research (IPSS).
Kawamoto H., Sankai Y. (2005), “Power assist method based on phase sequence and muscle force condition for HAL”, Advanced Robotics, vol. 19, no 7, p. 717-734.
Leikas J. (2014), Ikäteknologia, Raisio, NewPrint Oy.
Määttä H., Watanabe K., Miwa H. (2016), “Challenges of Integrating New Technology into Elderly Care Services – Perspectives of Service Provider Companies in Japan”, The 4th International Conference on Serviceology (ICServ2016). Tokyo, Japan, 6-8 September.
MHLW (2015), “About the supply-demand gap of elderly-care workforce toward 2025 (in Japanese)”, available at: http://www.mhlw.go.jp/file/04-Houdouhappyou-12004000-Shakaiengokyoku-Shakai-Fukushikibanka/270624houdou.pdf_2.pdf (accessed 13 July 2017).
Neumann D. (2016), “Human Assistant Robotics in Japan-Challenges and Opportunities for European Companies”, available at:
https://www.eu-japan.eu/sites/default/files/publications/docs/2016-03-human-assistant-robotics-in-japan-neumann_min_0.pdf. (accessed 27 March 2018)
Niemelä M., Watanabe K., Aaltonen I., Heikkilä P., Hyytinen K., Kulju M., Lammi H., Muhammad A., Määttä H., Tammela A., Ylikauppila M. (2017), “Meaningful technologies for seniors: comparing Finland and Japan”, in Leikas J. (Ed.), Ageing and technology, VTT Research Highlights 14, Helsinki. Juvenes Print.
121Obi T., Ishmatova D., Iwasaki N. (2013), “Promoting ICT innovations for the ageing population in Japan”, International Journal of Medical Informatics, vol. 82, no 4, p. 47-62.
OECD (2005), Long-term Care for Older People, Paris, OECD Publishing.
OECD (2013), A Good Life in Old Age? Monitoring and Improving Quality in Long-Term Care, Paris, OECD Publishing.
OECD (2017), Health at a Glance 2017: OECD Indicators, Paris, OECD Publishing.
Pieper R. (2002), “Introduction: The paradigm of gerontechnology”, in Pieper R., Vaarama M., Fozard J. L. (eds.), Gerontechnology. Technology and aging – starting into the third millennium, Aachen, Shaker Verlag, p. 2-14.
Rhee J. C., Done N., Anderson G. F. (2015), “Considering long-term care insurance for middle-income countries: comparing South Korea with Japan and Germany”, Health Policy, vol. 119, no 10, p. 1319-1329.
Sale P. (2018), “Gerontechnology, Domotics, and Robotics” in Masiero S., Carraro U. (eds.), Rehabilitation Medicine for Elderly Patients, Practical Issues in Geriatrics, Cham, Springer.
Scott W. R. (2001), Institutions and organizations, Thousand Oaks, CA, Sage.
Shibata T., Wada K. (2011), “Robot therapy: a new approach for mental healthcare of the elderly–a mini-review”, Gerontology, vol. 57, no 4, p. 378-386.
Shimizutani S. (2013), The Future of Long-term Care in Japan, RIETI Discussion Paper Series 13-E-064.
Siegel C., Hochgatterer A., Dorner, T. E. (2014), “Contributions of ambient assisted living for health and quality of life in the elderly and care services – a qualitative analysis from the experts’ perspective of care service professionals”, BMC Geriatrics, vol. 14, no 122.
Sugihara T., Fujinami T., Phaal R., Ikawa Y. (2015), “A Technology Roadmap of Assistive Technologies for Dementia Care in Japan”, Dementia, vol. 14, p. 80-103.
Sundbo J. (1997), “Management of innovation in services”, Service Industries Journal, vol. 17, no 3, p. 432-455.
Sundbo J., Gallouj F. (2000), “Innovation as a loosely coupled system in services”, International Journal of Services Technology and Management, vol. 1, no 1, p. 15-36.
Sun H., De Florio V., Gui N., Blondia C. (2009), “Promises and challenges of ambient assisted living systems”, The Sixth International Conference on Information Technology: New Generations 2009 (ITNG‘09). Las Vegas, NV, 27-29 April.
Teperi J., Porter M. E., Vuorenkoski L., Baron J. F. (2009), The Finnish health care system: a value-based perspective, Sitra reports 82.
THL, National Institute for Health and Welfare (2018): Social welfare and 122health care reform in Finland, available at: https://thl.fi/en/web/social-welfare-and-health-care-reform (accessed 19 February 2018)
Vargo S., Lusch R. (2004), “Evolving to a New Dominant Logic for Marketing”, Journal of Marketing, vol. 68, no 1, p. 1–17.
Vargo S., Lusch R. (2011), “It‘s all B2B…and beyond: Toward a systems perspective of the market”, Industrial marketing Management, vol. 40, p. 181–187.
Vargo S. L., Wieland H., Akaka M. A. (2015), “Innovation through institutionalization: A service ecosystems perspective”, Industrial Marketing Management, vol. 44, p. 63-72.
Wallin A., Harjumaa M., Pussinen P., Isomursu M. (2015), “Challenges of new service development: case video-supported home care service”, Service Science, vol. 7, no 2, p. 100–118.
Watanabe K., Mochimaru M. (2015), “Analysis on Collaborative Development of Meaningful Technologies in Services”, XXV RESER conference. Copenhagen, Denmark, 10-12 September, 2015.
Watanabe K., Niemelä M., Määttä H., Miwa H., Fukuda K., Nishimura T., Toivonen M. (2016), „Meaningful Technology for Seniors: Viewpoints for Sustainable Care Service Systems“, The 4th International Conference on Serviceology (ICServ2016). Tokyo, Japan, 6-8 September.
Watanabe K., Hyytinen K., Niemelä M. (2017), “Meaningful Technology for Seniors: Analytical Framework for Elderly-Care Service Systems”, The 5th International Conference on Serviceology (ICServ2017), Vienna, Austria, 12-13 July.
Windrum P., García-Goñi M. (2008), “A neo-Schumpeterian model of health services innovation”, Research Policy, vol. 37, no 4, p. 649-672.
Windrum P. (2013), “Multi-agent framework for understanding the success and failure of ServPPINs”, in Gallouj F., Rubalcaba L., Windrum P. (eds.), Public-private innovation networks in services, Cheltenham, Edward Elgar Publishing, p. 88-112.
Windrum P., Schartinger D., Rubalcaba L., Gallouj F., Toivonen M. (2016), “The co-creation of multi-agent social innovations: a bridge between service a social innovation re-search”, European Journal of Innovation Management, Emerald, vol. 19, no 2, p. 150-166.
Witell L., Kristensson P., Gustafsson A., Löfgren M. (2011), “Idea generation: customer co-creation versus traditional market research techniques”, Journal of Service Management, vol. 22, no 2, p. 140-159.
World Bank (2018), “World Bank Open Data”, available at: https://data.worldbank.org (accessed 19 February 2018)
1 Acknowledgement: We appreciate the sincere support by all the interviewees, and Minna Kulju from VTT. This study is supported by JST and Tekes in Strategic International Collaborative Research Program, SICORP.